
Opportunity
During any given week, there are 10 patients in our hospitals that suffer sepsis, one in five of whom will die.
A number of serious adverse events in the past twelve months and data from our Emergency Departments (ED) indicated we were not reliably recognising and treating patients with sepsis in a timely manner. Patients who presented to our EDs with sepsis were receiving antibiotics on average four hours into their presentation while international best practice specifies antibiotic should be administered within the first hour of diagnosis.
Our primary aim was to reduce inpatient mortality from sepsis to less than 15% by World Sepsis Day (31st August) 2017.
We aimed to do this through timely recognition, diagnosis and treatment of sepsis:
- better time to source control and antibiotics
- best recognition for potential to deteriorate
- brilliant infection care
We designed and executed an 18 month Survive Sepsis Improvement Collaborative with our Emergency Departments leading the way.
The collaborative consisted of four workstreams:
- Development of best practice guidelines by an expert advisory group
- Clinical education
- Ward based improvement initiatives
- Development of a measurement framework to track progress
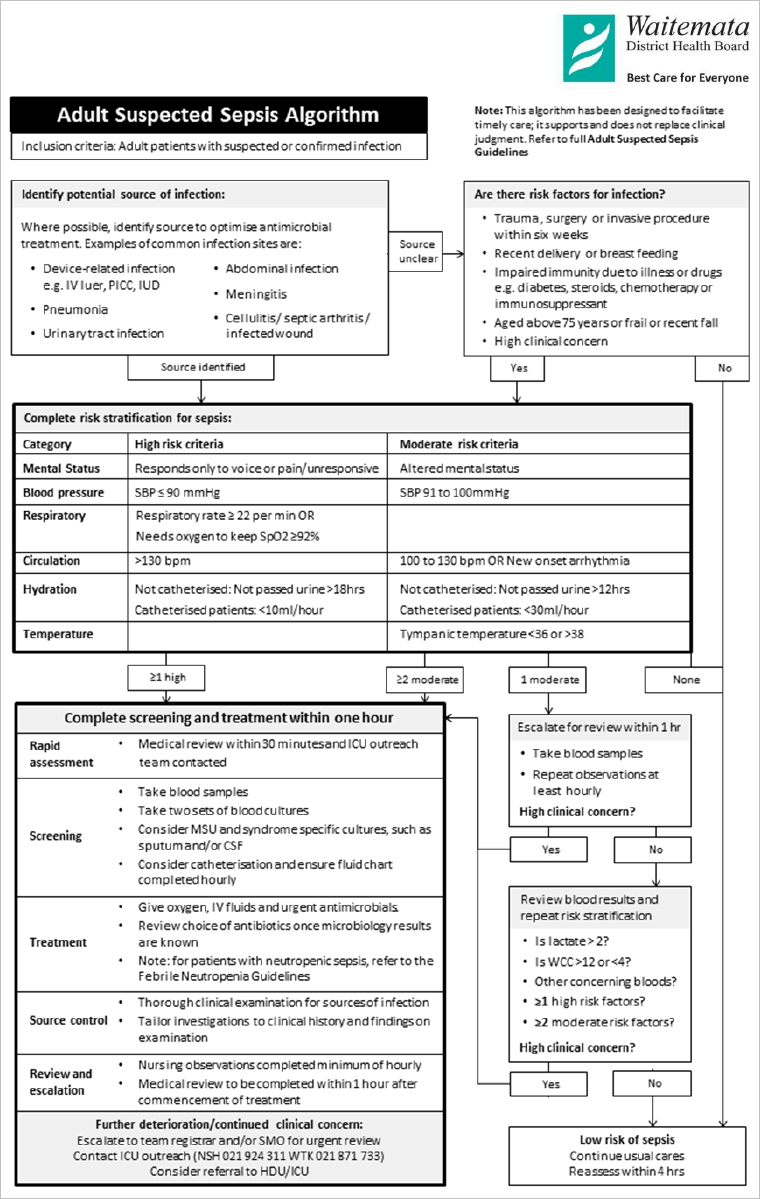
We developed Adult Inpatient Suspected Sepsis Guidelines, including a Suspected Sepsis Algorithm to guide staff through early recognition and treatment of suspected sepsis.
The guidelines include:
- Screening tools
- An escalation pathway based on patients’ clinical indicators and associated risk
- Treatment guidelines
- Measurement definitions

Suspected Sepsis Algorithm
In July 2017 we added a sepsis screening tool to the eVitals (PatientTrack) system. The sepsis screening tool compares vital signs to sepsis clinical indicators outlined in Waitemata DHB’s adult inpatient suspected sepsis guidelines.
Maternity and Paediatric guidelines are also under development.
We developed a sepsis clinical education package to support RN educators to deliver education to their ward areas and RMOs to their peers. We published the education package and guidelines on a sepsis intranet site and have been tracking visitor numbers during the project. The increase in visitors in June is consistent with an education drive before the introduction of the sepsis screening tool in eVitals.
We also developed a web based quiz via Kahoot to reinforce key learnings from our education package. Two hundred and eighty eight staff members have played the Waitemata DHB sepsis quiz. We have received some positive feedback about the quiz:
“Sepsis one was awesome. Short and succinct and ended with a good quiz”
“Love the quiz”

The Survive Sepsis Improvement Collaborative is based on the Institute for Healthcare Improvement’s (IHI) Breakthrough Series. The approach is designed to facilitate system wide improvements in quality by bringing multiple teams together for a short time to focus on improvements in a specific area.
We recruited 21 nurse (RN) and junior doctor (RMO) teams for each of our adult inpatient ward areas. We combined teams from clinically similar areas to create four groups. Each group was supported by an innovation and improvement project manager (i3PM) who guided the improvement process including application of improvement tools.
An improvement framework was designed to be applied learning over 6 months, building a strong foundational knowledge of quality improvement for all members of the team that can be applied to other future improvement projects:
| Timeline | Phases |
|
Jan |
Setting aims:
|
|
Feb-Mar |
Understanding the system
|
|
Apr-Jul |
Generate ideas and test
|
|
Aug-Sep |
Make it happen
|
The RN and RMO improvement leads tested four change ideas (eg a sepsis kit; sepsis escalation process) on our inpatient wards using the model for improvement.

Improvement Change Ideas
We will report against the following measures to understand the impact of our improvement activities on clinical practice and patient outcomes.

The measures will be added to a Qlik Sense dashboard to enable ward areas to track their management of patients with sepsis. We are also working with our health economist and data analysts to model and cost sepsis outcomes.
On 28th February 2017 nursing quality reps at North Shore and Waitakere hospitals completed a point prevalence audit. The purpose of the audit was to:
- identify a group of inpatients with suspected or confirmed sepsis
- understand the prevalence of sepsis within the general inpatient population
- gather more information to assist with improvement activity
The team reviewed 488 files from 18 inpatient wards. They identified 52 patients (11%) deteriorating from infection or identified as having sepsis.
We also analysed coded data to determine a baseline sepsis mortality rate and rate of admissions to ICU with sepsis.


Sepsis Outcome Measures
Prior to the improvement work we asked nurse and junior doctor improvement leads to rate their confidence with ten quality improvement and measurement tools on a 5-point likert scale. Mean baseline confidence rating was 2.8 out of 5 (range 1-4). Mean confidence rating after 4 months participation in the collaborative was 3.7 (range 2-5).

Building Quality Improvement Capability
- Survive Sepsis Improvement Collaborative (Poster)
- Survive Sepsis Driver Diagram
- Adult Suspected Sepsis Guidelines [May17]
- Suspected Sepsis Algorithm
- Survive Sepsis Kahoot Quiz
Survive Sepsis Improvement Ideas Posters
Sponsors
- Matt Rogers, Clinical Director of Laboratories
- Penny Andrew, Director of i3
- David Grayson, Clinical Director of Patient Safety + Patient Experience
- Shirley Ross, Head of Division Nursing, Specialist Medicine + Health of Older People Services
- Kate Gilmour, Head of Division Nursing, Surgical + Ambulatory Services
Clinical Advisory Team
- Hasan Bhally, Consultant Physician (Infectious Diseases)
- Jonathan Casement, Clinical Director ICU
- Chris Peterson, Paediatrician
- Amanda Holgate, Senior Medical Officer Emergency Medicine
- John Bottomley, Senior Medical Officer Radiology/Urology
- Anisha Sethi, Senior Medical Officer General Medicine
- Andrew Salmon, Senior Medical Officer Renal
- Andrew Moot, Surgeon, General Surgery
- Abir Abed-Ali, Senior Medical Officer Gynaecology
- Matt Rogers, Clinical Director Laboratories
- Nicola Williams, Pharmacy Team Leader
Improvement Teams
- i3 Innovation + Improvement Project Managers
- Registered Nurse + Junior Doctor Improvement Leads for each inpatient adult ward


{kind=link}